Diphtheria – a relatively easily-preventable infection – is evolving to become resistant to a number of classes of antibiotics and in future could lead to vaccine escape, warn an international team of researchers from the UK and India.
The researchers, led by scientists at the University of Cambridge, say that the impact of COVID-19 on diphtheria vaccination schedules, coupled with a rise in the number of infections, risk the disease once more becoming a major global threat.
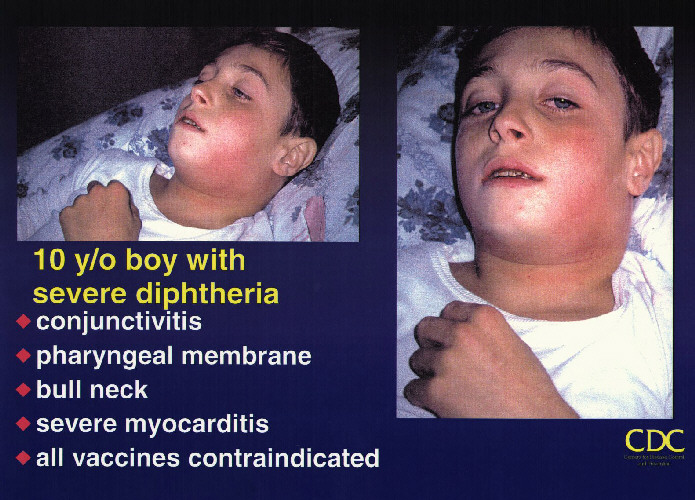
Diphtheria is a highly contagious infection that can affect the nose and throat, and sometimes the skin. If left untreated it can prove fatal. In the UK and other high-income countries, babies are vaccinated against infection. However, in low- and middle-income countries, the disease can still cause sporadic infections or outbreaks in unvaccinated and partially-vaccinated communities.
The number of diphtheria cases reported globally has being increasing gradually. In 2018, there were 16,651 reported cases, more than double the yearly average for 1996-2017 (8,105 cases).
Diphtheria is primarily caused by the bacterium Corynebacterium diphtheriae and is mainly spread by coughs and sneezes, or through close contact with someone who is infected. In most cases, the bacteria cause acute infections, driven by the diphtheria toxin – the key target of the vaccine. However, non-toxigenic C. diphtheria can also cause disease, often in the form of systemic infections.
In a study published today in Nature Communications, an international team of researchers from the UK and India used genomics to map infections, including a subset from India, where over half of the globally reported cases occurred in 2018.
By analysing the genomes of 61 bacteria isolated from patients and combining these with 441 publicly available genomes, the researchers were able to build a phylogenetic tree – a genetic ‘family tree’ – to see how the infections are related and understand how they spread. They also used this information to assess the presence of antimicrobial resistance (AMR) genes and assess toxin variation.
The researchers found clusters to genetically-similar bacteria isolated from multiple continents, most commonly Asia and Europe. This indicates that C. diphtheriae has been established in the human population for at least over a century, spreading across the globe as populations migrated.
The main disease-causing component of C. diphtheriae is the diphtheria toxin, which is encoded by the tox gene. It is this component that is targeted by vaccines. In total, the researchers found 18 different variants of the tox gene, of which several had the potential to change the structure of the toxin.

Professor Gordon Dougan from the Cambridge Institute of Therapeutic Immunology and Infectious Disease (CITIID) said: “The diphtheria vaccine is designed to neutralise the toxin, so any genetic variants that change the toxin’s structure could have an impact on how effective the vaccine is. While our data doesn’t suggest the currently used vaccine will be ineffective, the fact that we are seeing an ever-increasing diversity of tox variants suggests that the vaccine, and treatments that target the toxin, need to be appraised on a regular basis.”
Diphtheria infections can usually be treated with a number of classes of antibiotic. While C. diphtheriae resistant to antibiotics have been reported, the extent of such resistance remains largely unknown.
When the team looked for genes that might confer some degree of resistance to antimicrobials, they found that the average number of AMR genes per genome was increasing each decade. Genomes of bacteria isolated from infections from the most recent decade (2010-19) showed the highest average number of AMR genes per genome, almost four times as many on average than in the next highest decade, the 1990s.
Robert Will, a PhD student at CITIID and the study’s first author, said: “The C. diphtheriae genome is complex and incredibly diverse. It’s acquiring resistance to antibiotics that are not even clinically used in the treatment of diphtheria. There must be other factors at play, such as asymptomatic infection and exposure to a plethora of antibiotics meant for treating other diseases.”
Erythromycin and penicillin are the traditionally recommended antibiotics of choice for treating confirmed cases of early-stage diphtheria, though there are several different classes of antibiotics available to treat the infection. The team identified variants resistant to six of these classes in isolates from the 2010s, higher than in any other decades.
Dr Pankaj Bhatnagar from the World Health Organization country office for India said: “AMR has rarely been considered as a major problem in the treatment of diphtheria, but in some parts of the world, the bacterial genomes are acquiring resistance to numerous classes of antibiotics. There are likely to be a number of reasons to this, including exposure of the bacteria to antibiotics in their environment or in asymptomatic patients being treated against other infections.”
The researchers say that COVID-19 has had a negative impact on childhood vaccination schedules worldwide and comes at a time when reported case numbers are rising, with 2018 showing the highest incidence in 22 years.
Dr Ankur Mutreja from CITIID, who led the study, said: “It’s more important than ever that we understand how diphtheria is evolving and spreading. Genome sequencing gives us a powerful tool for observing this in real time, allowing public health agencies to take action before it’s too late.
“We mustn’t take our eye off the ball with diphtheria, otherwise we risk it becoming a major global threat again, potentially in a modified, better adapted, form.“










{kind=link}
We already know how to kill bacteria. Why the expensive and Quixotic gene therapy/vaccination focus? Colloidal silver is all you need. Inexpensive, reliable and readily available. There are dozens of other effective natural antibiotics. Then there’s hypochlorous acid, which you can make yourself if need be. The focus on vaccines seems to me to be politically motivate, to keep people under control and dependent upon the thoroughly corrupt medical mafia.